Hey, User !
Hey, User !
Welcome to SayaCare! 👋FREE delivery on 1st order — Use coupon: TESTME101
Here's a guide 📝 to safely buying medicine online.

Follow Us For More





Content Writer
Published on 11-6-2025
•6 min read

As a trained economist who runs an E-pharmacy the National Pharmaceutical Pricing Authority (NPPA) of India is an example of how government institutions can legitimize the worst tendencies of the free market. In this blog, I will establish a few key points
If you are interested in public-policy and pharmaceuticals, then this blog is for you. Otherwise, my fair pharmacist/doctor/patient/caregiver – there are other insightful reads for you on our website.
Free Market is not an Optimal Market
A free-market is one where there is a voluntary exchange between buyers and sellers. However, in order for a market to be optimal – buyers and sellers must have complete transparency and information.
Medicine has no transparency, as the buyer has close-to-zilch information. Nearly all patients are so far out of the loop, that they are dependent on an authority figure to make this decision for them.[1][1]
In this environment, an individual needs guidance, and there is limited/if any accountability over what the doctor prescribes and what benefit they derive from it. With near-absolute information asymmetry and absolute emotional pandemonium[2], doctors and companies exploit ignorant patients.
As discussed by Mahak, most of the pricing of medicine goes into its marketing cost through information asymmetry exploiting means. The top-selling pharmaceutical brands of every molecule are sold in this manner.
NPPA makes Astronomical Prices Seem Sensible
All of us exclusive “Trade-Generic” types, account for roughly 5000 Cr out of 232400 Cr market (2.5% of value – 5% of volume). Trade-Generics are generic-medicine which are sold through substitution instead of direct prescribing. However, most generics are sold via traditional general-chemist shops which IQVIA estimates at 15-20% of volume and 5% of value[3]. This 5% of value is split amongst so many different pharmaceutical marketing companies, that barely any company has any significant market share. This is an extremely important point – none of these trade-generic companies has even a fraction of a percent[4].
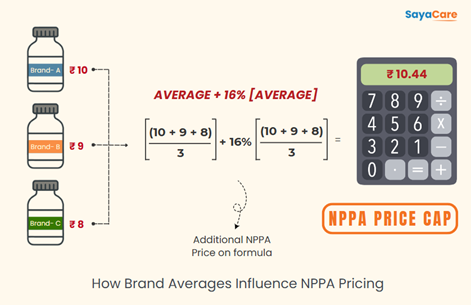
The NPPA calculates the maximum price by taking the average of the top pharmaceutical brands and adding 16% on top of that[4]. Top Pharmaceutical brands are determined by the All India Organization of Chemists and Druggists through their Pharma rack System as having over 1% market share. Trade-generics with their already low volume and spread through so many different *brands* – would never be classified as having over 1% market share[5].
To clarify suppose molecule X has 3 companies with 1% market share. Say the MRP of these drugs is: 10, 9, & 8. This makes the average (10 + 9 + 8) / 3 = 9 with a 16% increase resulting in the final NPPA price being Rs. 10.44.
The NPPA sets the Maximum Retail Price for Brands, Trade-Generics by the very disperse nature of their sale – are never counted.
Ramifications
The NPPA limit makes astronomical prices seem sensible. If a medicine costs Rs. 10 to make, but every major brand is selling around Rs. 400 – then the NPPA price will be set around Rs. 400. The trade-generic players didn’t even get factored in. Consumers view that the price is near the Government-Mandated price, and think this is a fair price.
Market manipulation through volume/price control is common. Ecosprin 75 mg(Aspirin 75 mg (Acetyl Salic Acid 75 mg)) is completely controlled by USV, one of the original Indian manufacturer/marketers, which has a near monopoly on the plain Aspirin market in India. Due to this, they have the set price so low as to not allow any competition. Medicine requires scale to be profitable – they have set it such a low price that new competition cannot rise. It is like China dumping its steel in India so that no domestic steel manufacturer can get large enough to compete. This might seem efficient to the consumer, but if USV files bankruptcy – India is out of Aspirin.
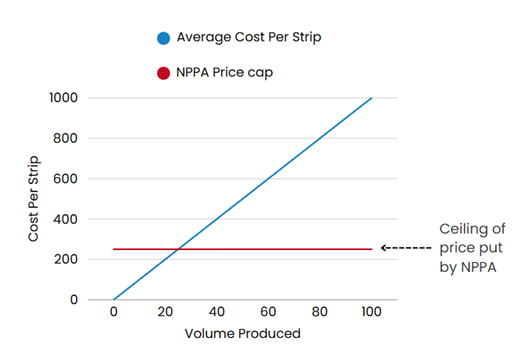
Graph 1: NPPA Impact on Supply Curve
Graph 2: Supply-Chain Shocks
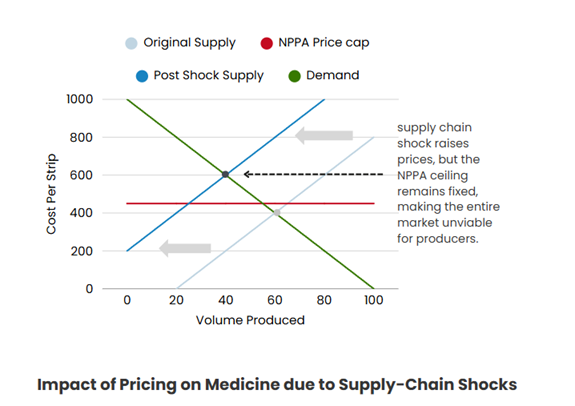
This is outlined in Graph 1 & 2, wherein a supply chain shock raises the price, causing the medication to be inappropriately priced thereby making the market unviable for producers.
The market frequently needs to adjust to shocks to the system. Think some crucial mines making a raw ingredient for an API (Salt) got flooded, and prices have risen dramatically. The free-market causes prices of manufacturing to rise – the NPPA does not keep pace. The drug becomes unprofitable to manufacture. This has frequently occurred as can be seen by the number of drugs regulated by the NPPA that are no longer sold in India.11 This phenomenon mostly occurs on Brand Monopolies as they are the ones that would bring prices so low as to bring out the worst in government controls on pricing.
Benefits
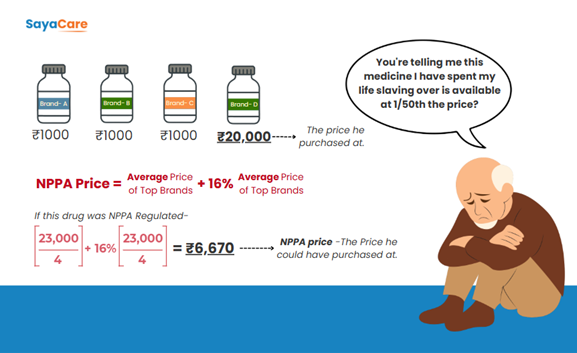
There is actually just one scenario I can think of, where the current NPPA system protects against. A company comes in with absolute disregard for the financial health of its patients. The company realizes that with enough information asymmetry they can convince some fellow out there to pay 10000x what the medicine should cost using some bogus line that its “imported from Denmark”. This occurs more than I’d like to admit, with one notable door-to-door encounter early in the company history resulting in an old man crying as he realized his life-long debt had been due to a scam like this.
If that drug had been regulated by the NPPA, then such a scam could never occur – as most companies do not exploit information asymmetry to such an extreme, and the average would be set considerably lower.
Conclusion
Beyond the limitation of scope, the NPPA reinforces monopolies, misleads consumers, and occasionally dismantles the distribution of certain medication. The only legitimate protection it offers is against a very rare ailment in the market.
There are two options to fix the market.
Since the latter is out of our hands, SayaCare strives to do the former. SayaCare wants to build a world where healthcare is easy. That means the patient has complete information, and their authority figures guide them with an alignment in interests.
The more educated the populace is on how drugs are made, sold, work, stored, and so-forth – the better they can choose for themselves what is required. That’s why we write blogs and produce reels. We believe when the patient has complete information and the healthcare provider have the right incentives/accountability – truly effective healthcare can take place.
[1] IE. A Doctor.
[2] When illness strikes, you do not question the pricing of the remedy – you need a remedy, whatever the cost.
[3] https://www.iqvia.com/-/media/iqvia/pdfs/india/winning-in-the-indian-pharmaceutical-market.pdf?_=1610873724999
[4]https://pharma-dept.gov.in/sites/default/files/dpco2013gaz.pdf
[5] Except perhaps the Jan Aushadhi, but they don’t factor into the AICOD’s Pharmarack system.
This critique of government medicine pricing in India is eye-opening. The core argument—that the NPPA’s formula, which sets price caps based on the average of the most expensive top brands, essentially legitimizes astronomical prices and ignores cheaper alternatives—is a powerful point. Furthermore, the article highlights how this rigid control can accidentally reinforce monopolies and lead to drug shortages when market shocks make a capped price unprofitable for manufacturers. It seems the author advocates for greater patient transparency over rigid administrative price ceilings.